
Elbow pain is a frequent complaint among adults, significantly affecting daily activities such as lifting, gripping, typing, or even simple household tasks. Two of the most common conditions responsible for persistent elbow discomfort are Tennis Elbow (Lateral Epicondylitis) and Golfer’s Elbow (Medial Epicondylitis). Despite their names, these conditions are not limited to athletes. They frequently affect anyone engaging in repetitive arm and wrist movements in work, sports, or daily life.
The Anatomy Behind Elbow Pain
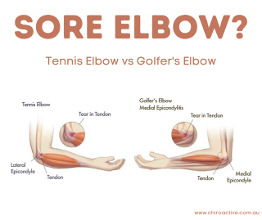
The elbow functions as a hinge joint, allowing bending, straightening, twisting, and gripping motions. Surrounding muscles of the forearm attach via tendons to bony landmarks on either side of the elbow.
- Tennis Elbow (Lateral Epicondylitis) results from overuse of the wrist extensor muscles, particularly the extensor carpi radialis brevis, where it inserts on the lateral epicondyle (outer elbow). Repetitive strain leads to microtears and degenerative changes within the tendon tissue.
- Golfer’s Elbow (Medial Epicondylitis) involves the wrist flexor-pronator group, which inserts at the medial epicondyle (inner elbow). Activities requiring repetitive wrist flexion or forearm pronation often contribute to tendon overload.
Both conditions typically develop gradually over time due to repeated microtrauma rather than a single traumatic event.
Who Is at Risk?
Both Tennis Elbow and Golfer’s Elbow may affect individuals who:
- Perform repetitive manual tasks (e.g., gardening, painting, plumbing, carpentry).
- Spend extended periods using computers or performing desk work.
- Engage in weightlifting or repetitive gym workouts.
- Repeatedly lift or carry children.
- Participate in racket sports, golf, or similar repetitive arm motions.
These conditions are most prevalent among individuals aged 35 to 55, though they may occur at any age depending on activity level.
Clinical Presentation: What Does It Feel Like?
| Tennis Elbow (Lateral Epicondylitis) | Golfer’s Elbow (Medial Epicondylitis) |
| Pain on the outer elbow | Pain on the inner elbow |
| Worsens with gripping, lifting, wrist extension | Worsens with wrist flexion, gripping, forearm pronation |
| Weak grip strength | Reduced forearm strength |
| Stiffness, tenderness with pressure | Stiffness with wrist movement |
Initially, discomfort may only occur during physical activity, but if untreated, it can progress to constant pain even at rest.
The Importance of Early Intervention
Timely treatment is critical. Delayed care allows microtears to accumulate, potentially leading to chronic tendon degeneration (tendinosis), increased stiffness, and prolonged recovery times. Early intervention can help restore function quickly and minimize long-term disability.
Evidence-Based Treatment Options
Fortunately, most cases respond well to conservative treatment without requiring surgery.
Manual Therapy & Physiotherapy
- Soft tissue mobilization, friction massage, and manual therapy to improve tendon health.
- Joint mobilisations to restore range of motion and reduce mechanical stress.
- Taping or bracing may temporarily reduce tendon load during activity.
Which Exercises Should I Use for Tennis Elbow and Golfer’s Elbow?
Strengthening the muscles and tendons surrounding the elbow joint is essential for recovery, injury prevention, and long-term tendon health. Below are specific exercises targeting key muscles involved in Tennis Elbow (lateral epicondylitis) and Golfer’s Elbow (medial epicondylitis).
For Tennis Elbow (Lateral Epicondylitis)
Wrist Extensors (Extensor Carpi Radialis Brevis & Longus)
Wrist Extensor Stretch
- Extend your arm fully in front of you with the palm facing down.
- Use your opposite hand to gently pull your wrist down, stretching the top of the forearm.
- Hold for 20–30 seconds.
- Repeat 3–5 times daily.
Eccentric Wrist Extension with Dumbbell
- Sit with your forearm supported on a table, palm facing down.
- Hold a light dumbbell (0.5–2 kg).
- Use your non-affected hand to lift your wrist into full extension.
- Slowly lower the wrist down into flexion over 3–5 seconds (eccentric phase).
- Repeat 10–15 repetitions, 3 sets.
Isometric Wrist Extension
- Place your forearm on a table, palm facing down.
- Push your hand upward against a stable surface (or therapist hand) without moving the wrist.
- Hold for 10 seconds.
- Perform 10 repetitions.
Grip Strengthening
- Hold a soft rubber ball or hand therapy putty.
- Squeeze and hold for 5–10 seconds.
- Perform 10–15 repetitions, gradually increasing resistance over time.
For Golfer’s Elbow (Medial Epicondylitis)
Wrist Flexors (Flexor Carpi Radialis, Flexor Carpi Ulnaris, Pronator Teres)
Wrist Flexor Stretch
- Extend your arm fully in front of you with the palm facing up.
- Use your opposite hand to gently pull your fingers and wrist backward, stretching the inside of your forearm.
- Hold for 20–30 seconds.
- Repeat 3–5 times daily.
Eccentric Wrist Flexion with Dumbbell
- Sit with your forearm supported on a table, palm facing up.
- Hold a light dumbbell (0.5–2 kg).
- Use your non-affected hand to lift your wrist into full flexion.
- Slowly lower the wrist down into extension over 3–5 seconds.
- Repeat 10–15 repetitions, 3 sets.
Isometric Wrist Flexion
- Place your forearm on a table, palm facing up.
- Press your palm upward into a stable surface without moving your wrist.
- Hold for 10 seconds.
- Perform 10 repetitions.
Forearm Pronation and Supination with Resistance Band
- Attach a resistance band to a fixed object.
- Hold the band with your elbow bent at 90 degrees, palm facing sideways.
- Rotate your forearm inward (pronation) and outward (supination) slowly.
- Perform 10–15 repetitions each direction, 2–3 sets.
Grip Strengthening
- Hold a soft rubber ball or hand therapy putty.
- Squeeze and hold for 5–10 seconds.
- Perform 10–15 repetitions, gradually increasing resistance over time, focusing on slow controlled squeezes.
Proximal Stability: Shoulder & Scapular Control (Important for both conditions)
Scapular Retractions (Postural Control)
- Stand upright, arms by your sides.
- Gently pinch your shoulder blades together.
- Hold for 5–10 seconds.
- Repeat 10–15 times.
Wall Angels
- Stand against a wall with your back, head, and arms flat against the wall.
- Slowly raise and lower your arms like making a “snow angel”, keeping elbows and wrists in contact with the wall.
- Perform 10 repetitions.
Important:
Always perform exercises with proper form. Progress slowly with weight or resistance. Stop any exercise if it provokes sharp or prolonged pain. A physiotherapist should supervise your exercise progression to ensure safety and optimal recovery.
Activity Modification & Ergonomics
- Posture correction, improved lifting technique, and ergonomic adjustments for workstations.
- Activity pacing and load management to reduce repetitive strain during daily tasks.
Advanced Modalities
- Shockwave therapy, ultrasound, and dry needling may be beneficial in selected cases.
- Injections (e.g., corticosteroids or platelet-rich plasma) are rarely necessary and typically reserved for stubborn cases.
- Surgery is considered a last resort after failed conservative care over at least 6–12 months.
Recovery Timeline
With consistent care, most individuals experience significant improvement within 6 to 12 weeks. Severe or chronic cases may require a longer period of rehabilitation, but full recovery is achievable for most patients.
Prevention Strategies
Preventing recurrence or future injury is possible by adopting these key habits:
- Warm up properly before activities.
- Perform regular forearm stretches.
- Build strength in wrist extensors, flexors, and grip muscles.
- Apply proper lifting techniques.
- Take breaks from repetitive tasks to allow recovery.
Strengthening and balancing the muscles around the elbow reduces strain on the tendons and protects against overuse.
Take Action Early
If you’re experiencing any of these symptoms, don’t wait or hope it will simply resolve on its own. Early care makes treatment easier and recovery faster, allowing you to return to your daily activities without pain.
We’re here to help. At Rise Physio, we take the time to listen, assess, and create a treatment plan designed for you, not just your symptoms.
Book your personal assessment today and let’s get you back to moving pain-free.